
Right Ventricular Dimension
1. Right Ventricular Size
RV dilatation often associated (although not always) with acute pressure overload. Common pathologies includes acute pulmonary embolism and RV failure.
1.1 Subjective assessment (or what the experts called "eyeballing")
View: A4C (right ventricle-focused view)
Phase: end diastole (where chamber size at max)
Nothing fancy, just a simple pattern recognition. In normal person:
- RV size should be smaller than the LV, (by a ratio of less than 0.6 to be exact)
- LV should make up all the apex of the heart.
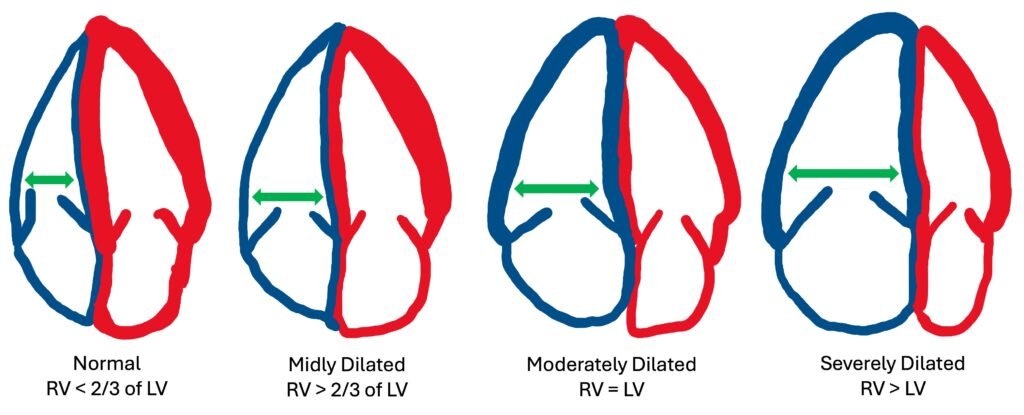
Image 1: RV dilatation based on it’s size compared to LV
1.2 Specific measurement of RV dimension / diameter
View: A4C (right ventricle-focused view)(see link)
Phase: end diastole (where chamber size at max)
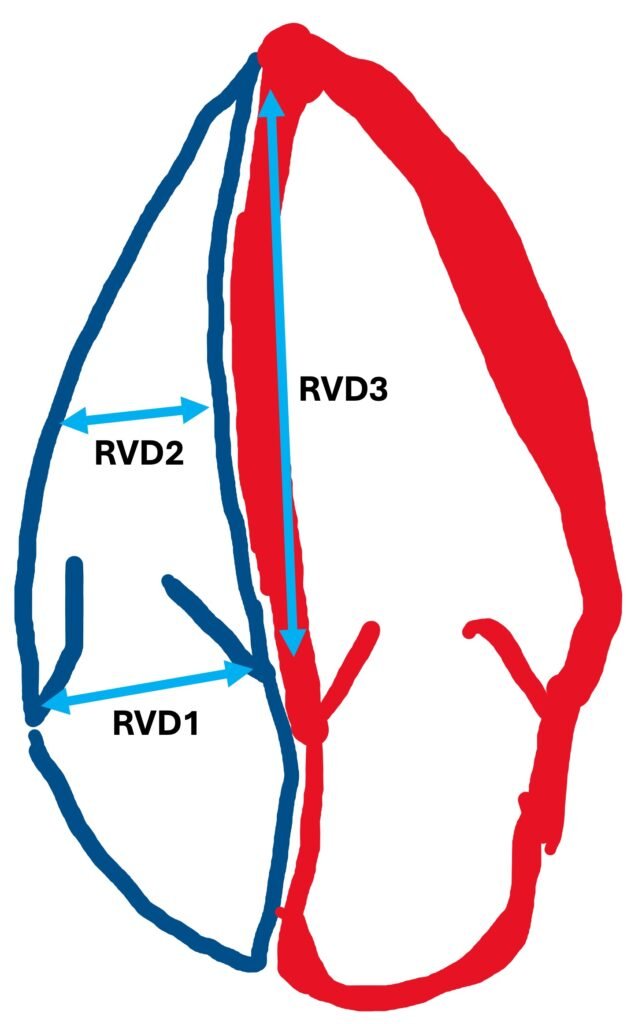
Image 2: Measurement of RV
Basal diameter (RVD1): maximal short axis dimension in the basal 1/3 of RV
Mid-cavity diameter (RVD2): diameter of RV at the level of LV papillary muscles
Longitudinal dimension (RVD3): distance from plane of tricuspid annulus to apex of RV
Normal values:
RVD1: < 4.2 cm
RVD2: < 3.5 cm
RVD3: < 8.6 cm
In summary, RV dilatation can be summarised into 3 main categories as below:
Mild | RV basal diameter < 4.2 cm, but LV still appear larger than RV |
Moderate | RV is approximately the size of LV (RV/LV ratio > 0.6) |
Severe | RV is larger than LV (RV/LV ratio > 1.0) RV forms the whole apex of the heart |
RV/LV ratio is known to be a strong predictor of adverse clinical outcomes and / or hospital mortality in patient with acute PE.
2. Right Ventricular Wall Thickness
RV hypertrophy can be a sign of chronic RVSP overload, infiltrative and hypertrophic cardiomyopathies.
View: PLAX or subcostal +/- M mode
Phase: end diastole (where chamber size at max)
Measurement can be done using PLAX or subcostal view, and with or without using the M mode. It is essential to ensure that trabeculations (from the endocardial border) and epicardial fat (from epicardial border) are excluded during measurement.
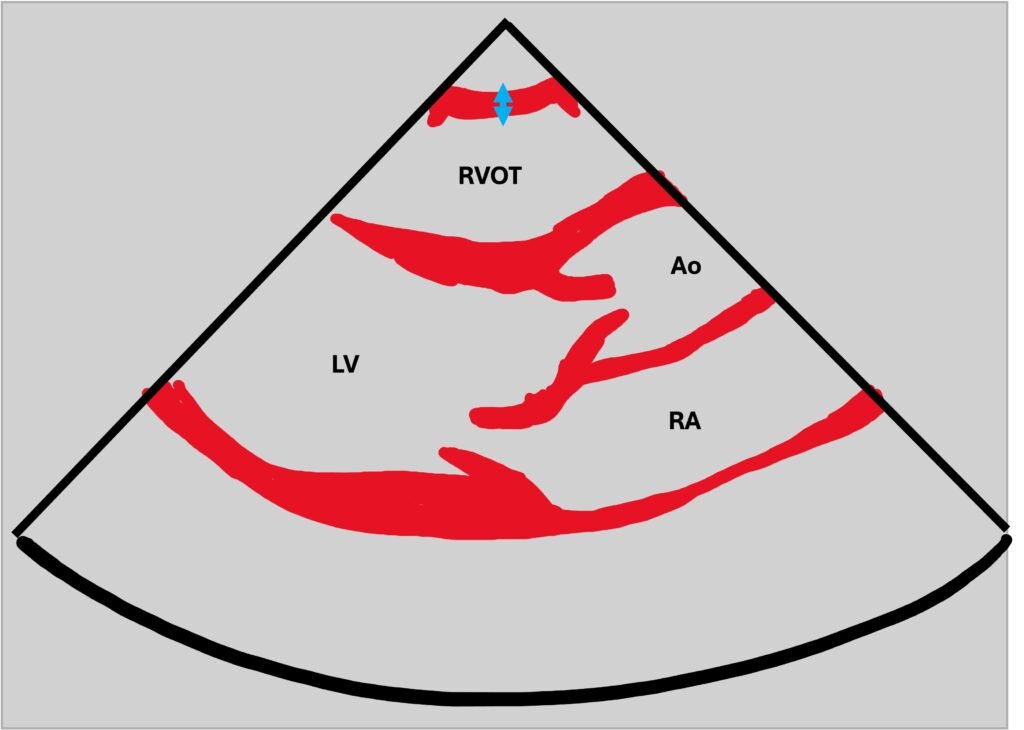
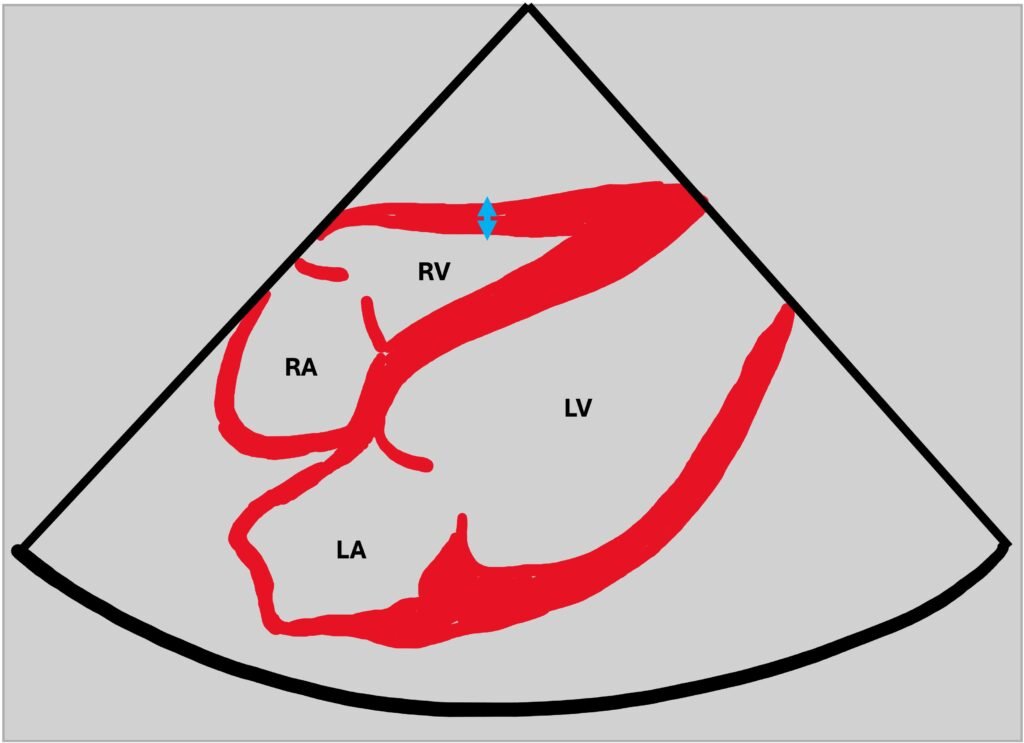
Image 3 & 4: RV wall thickness (blue arrow) in PLAX and subcostal view
Normal value: < 0.5 cm
3. Extras
These are not really part of the rapid assessment or focus bedside echo, but they are pretty simple and quick to do, just to add up to your overall assessment.
3.1 The rule of thirds
View: PLAX
Phase: end diastole
The RV, aorta and LA should be roughly the same size. You can suspect an RV enlargement if the RVOT segment is noticeably larger than the aorta / LA. Although you might missed this sign if the other 2 chambers dilated along with the RV.
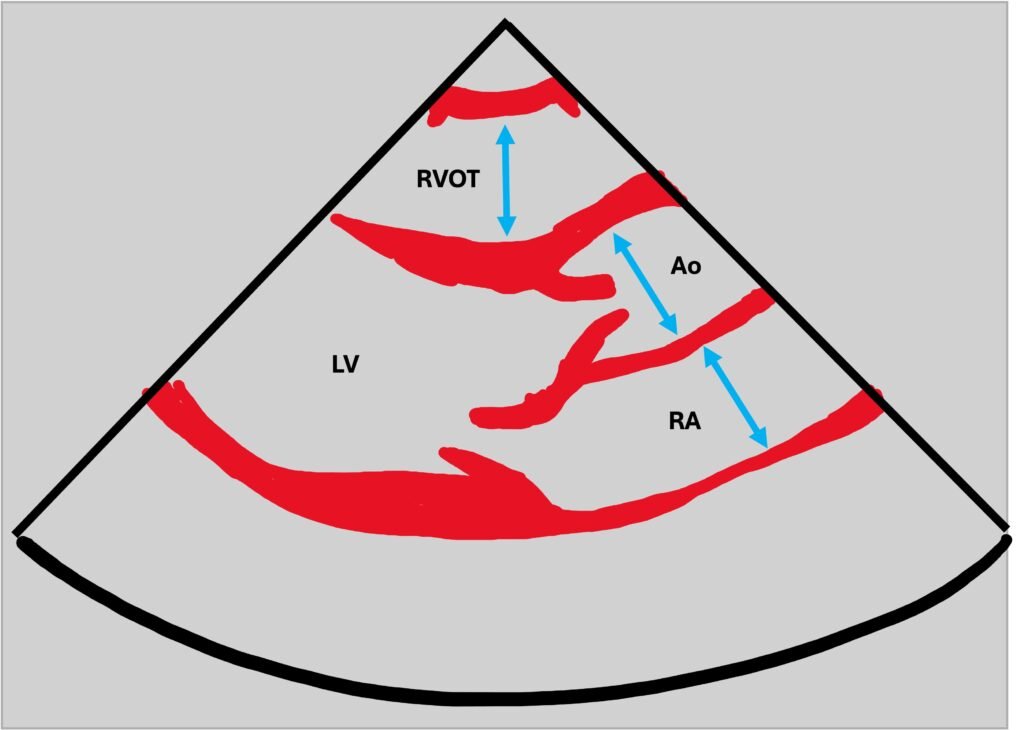
Image 5: PLAX view showed the RVOT, aorta and right atrium ratio of 1:1:1
References:
- Anthony McLean et al. Oxford Textbook of Advanced Critical Care Echocardiography. UK: Oxford University Press; 2020
- Rudski LG, Lai WW, Afilalo J, Hua L, Handschumacher MD, Chandrasekaran K, et al. Guidelines for the echocardiographic assessment of the right heart in adults: a report from the American Society of Echocardiography. J Am Soc Echocardiogr. 2010 Jul;23(7):685-713. Available from: www.onlinejase.com
- Lang RM, Badano LP, Mor-Avi V, Afilalo J, Armstrong A, Ernande L, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr. 2015 Jan;28(1):1-39.e14. Available from: www.asecho.org
- Schneider M, Aschauer S, Mascherbauer J, Adelbrecht C, Beitzke D, Binder C, et al. Echocardiographic assessment of right ventricular function: current clinical practice. Int J Cardiovasc Imaging. 2019;35(1):49-56. Available from: www.ncbi.nlm.nih.gov
- Pavlicek M, Wahl A, Rutz T, de Marchi SF, Hille R, Wustmann K, et al. Right ventricular systolic function assessment: rank of echocardiographic methods vs. cardiac magnetic resonance imaging. Eur J Echocardiogr. 2011 Nov;12(11):871-80. Available from: academic.oup.com
- Zornoff LA, Skali H, Pfeffer MA, St John Sutton M, Rouleau JL, Lamas GA, et al. Right ventricular dysfunction and outcomes in myocardial infarction: the SAVE experience. J Am Coll Cardiol. 2002;39(9):1450-5. Available from: www.jacc.org
Recent Posts
- Right Ventricular Dimension February 27, 2026
- Pneumothorax – CXR February 10, 2026
- The Three Planes / Views January 16, 2026
- The Hounsfield Unit, Window Level & Width January 16, 2026
- THE BLIND MEN & THE ELEPHANT January 14, 2026