
Pulmonary Embolism
What’s normal ?
For further details on CTPA please see specific section on CTPA and CT angiogram. In summary, the contrast helps to enhance the outline of the vessels.
The normal CTPA has continuous flow of hyper-attenuated contrast within the vasculature of pulmonary artery (PA) and its branches.
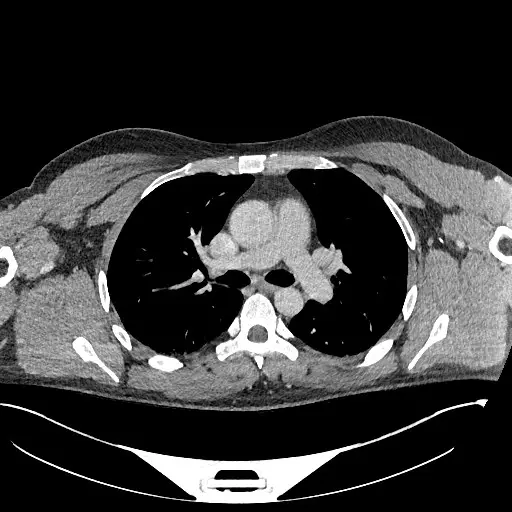
Figure 1: CT chest without contrast
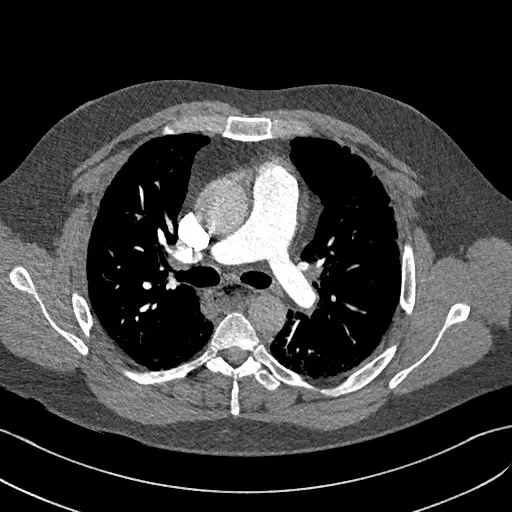
Figure 2: CTPA with contrast within the bifurcation of the main PA
What’s not normal ?
We should start from the pulmonary trunk (use axial view) and browse through each of the segment and sub-segment branches to look for filling defect. This is the low attenuation area within the contrast-enhanced lumen.
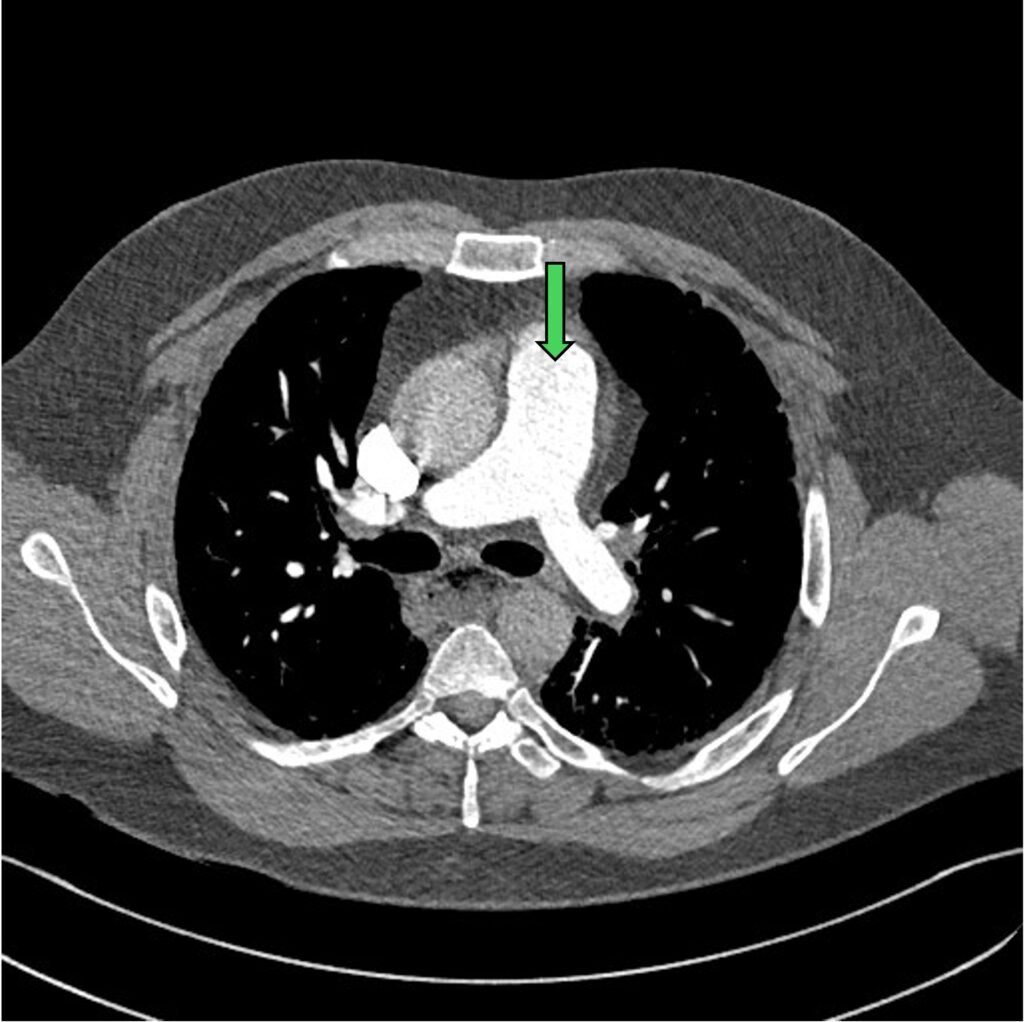
Figure 3: pulmonary trunk (green arrow) with bifurcation to left and right main PA
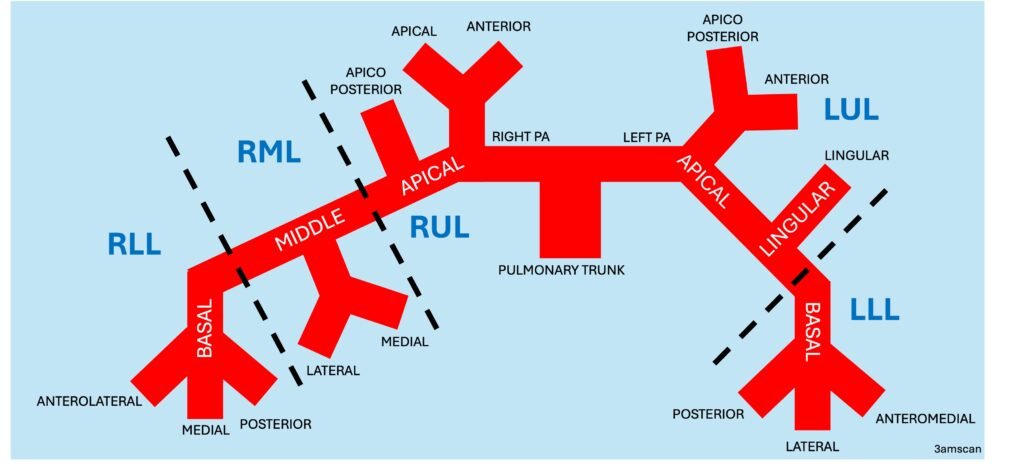
In this situation, it does help to be familiar with the PA anatomy and its branches. Below is the crude schematic diagram of the main PA and its branches.
The filling defect can be divided into occlusive vs. non-occlusive.
The non-occlusive filling defects will have a thin stream of contrast next to the clot, within the lumen of the vessel.

Figure 4: near occlusive clot in both the right and left main PA
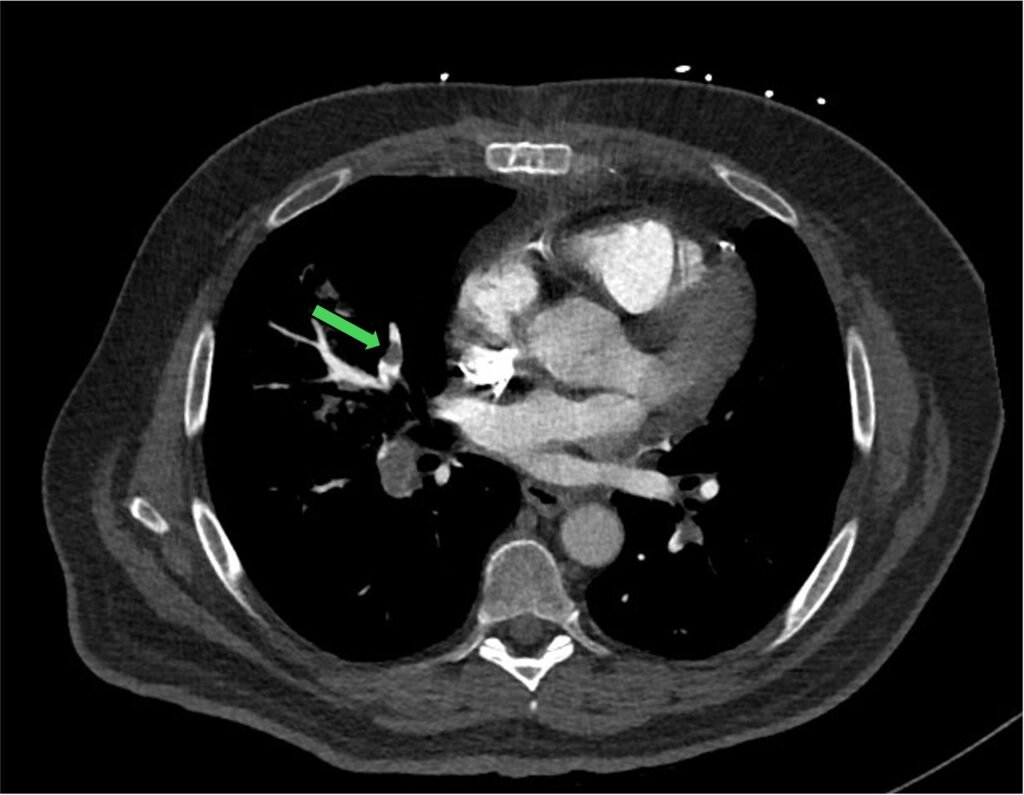
Figure 5: non-occlusive clot in one of the segments of right PA
Sometimes the formation of clots is so extensive, you can see a saddle shape clot within the bifurcation of the pulmonary trunk. This (saddle PE) is often associated with high clot burden and RV strain.
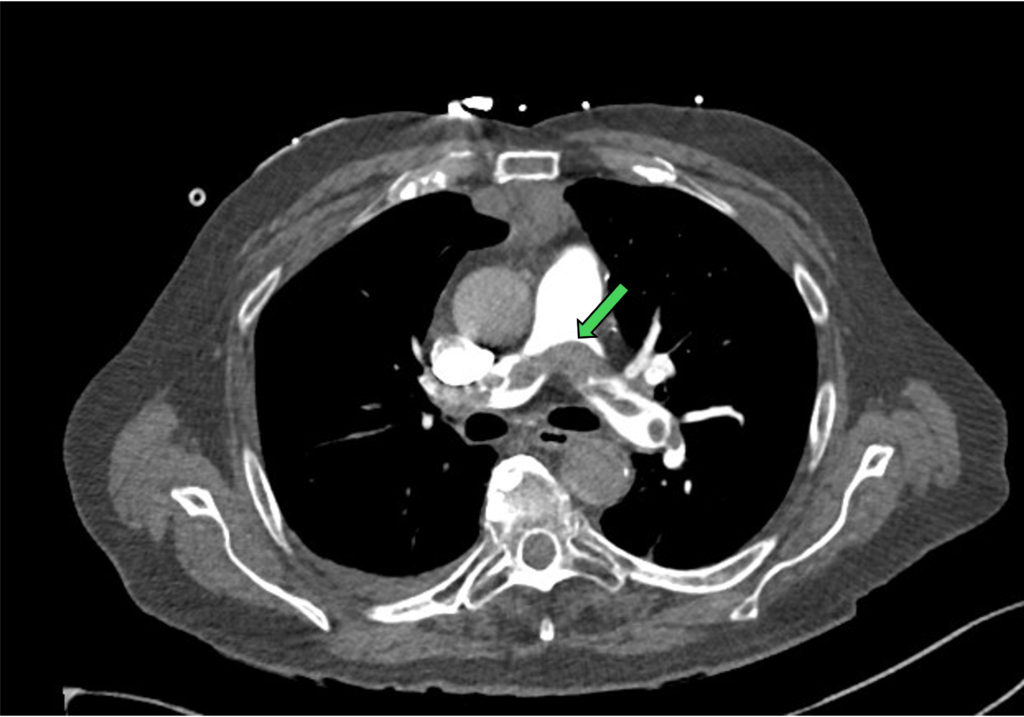
Figure 6: saddle PE (green arrow)
Other typical signs of PE are the polo mint sign and railway track sign.
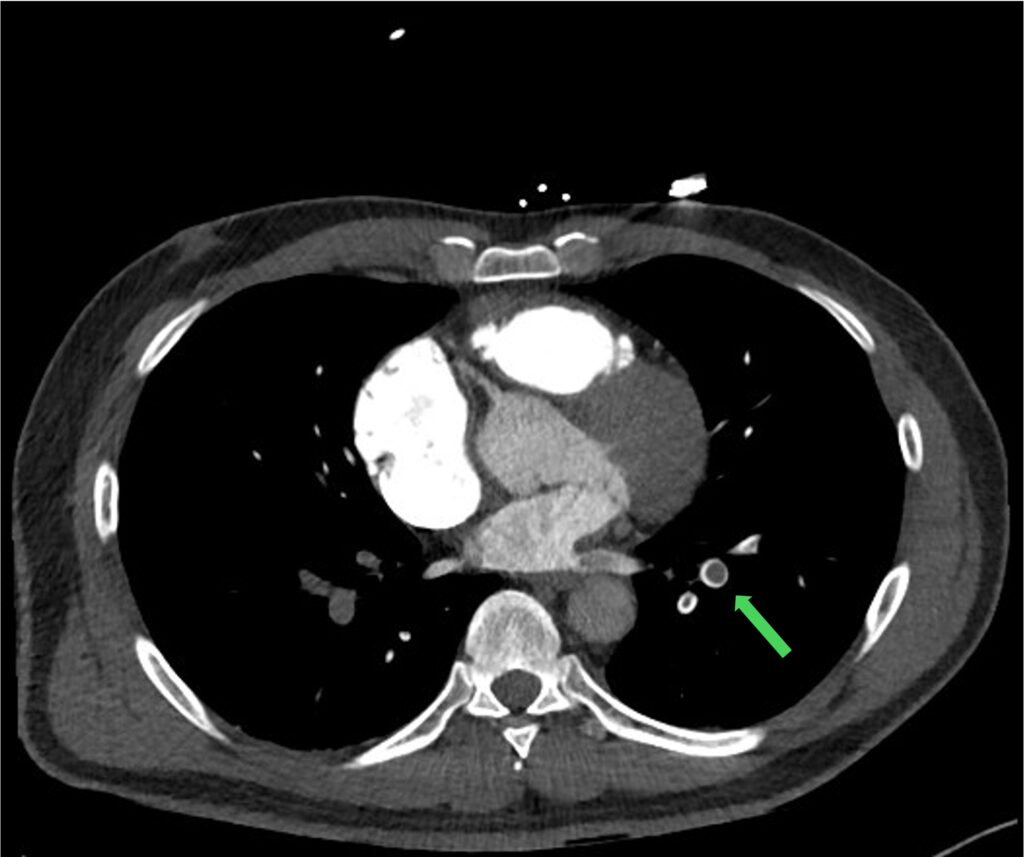
Figure 7: polo mint sign: central filling defect surrounded by ring of contrast (usually found on axial view)
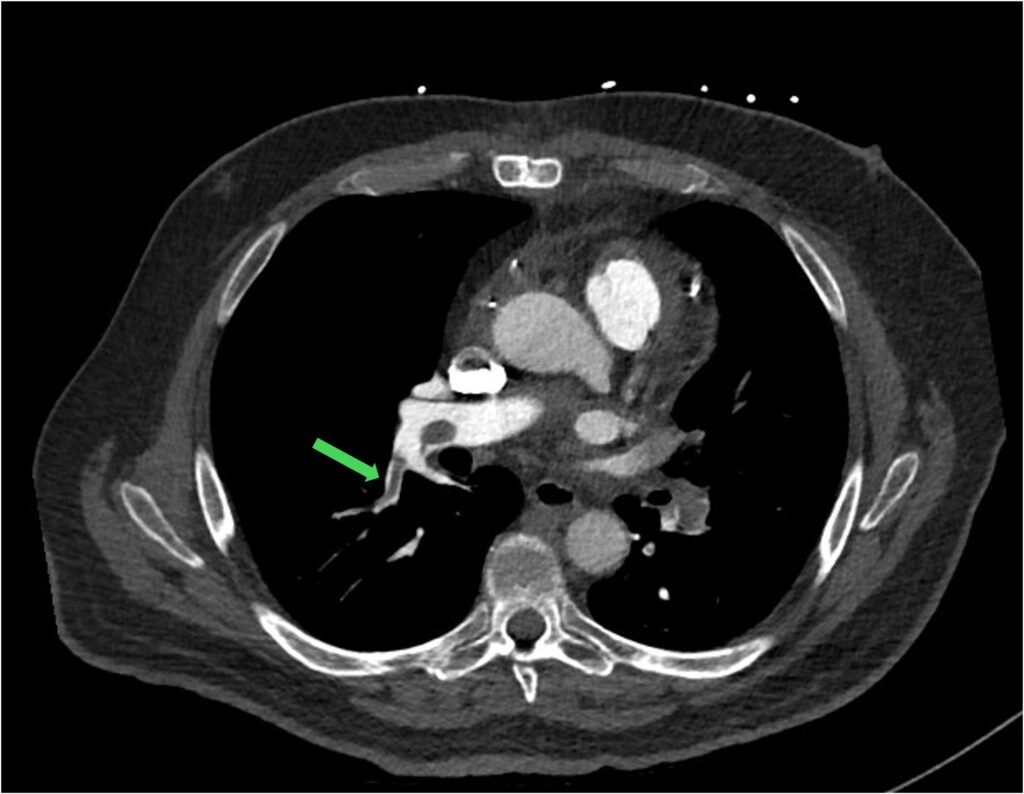
Figure 8: railway track sign: central filling defect surrounded by parallel lines of contrast
We should also look for the complications of PE.
When the clot burden is high, it can often put a strain on the RV. This is really one of the things that you don’t want to miss. Main features includes:
- enlarged RV with RV:LV ratio > 1
- flatenning or bowing of the intraventricular septum
- PA enlargement (> 2.9 cm)
- contrast reflux to IVC and hepatic vein
Do know that the last 2 features are less reliable and can be a chronic changes such as in pulmonary hypertension.
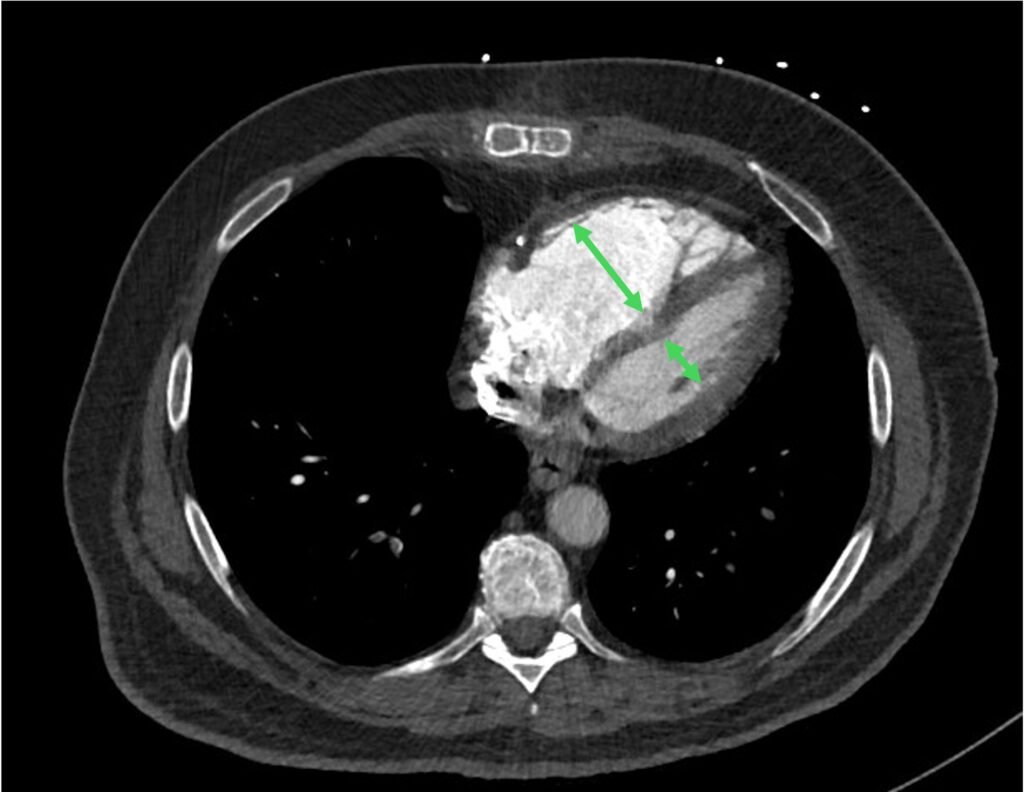
Figure 9: enlarged RV with RV:LV ratio > 1
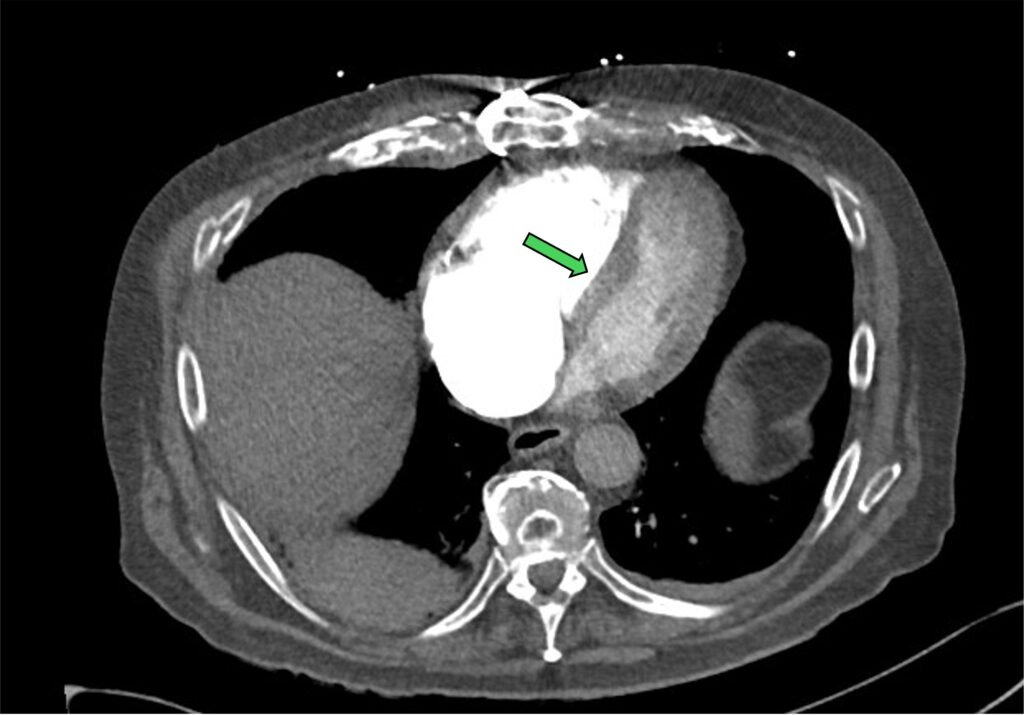
Figure 10: flattening / bowing of the intraventricular septum
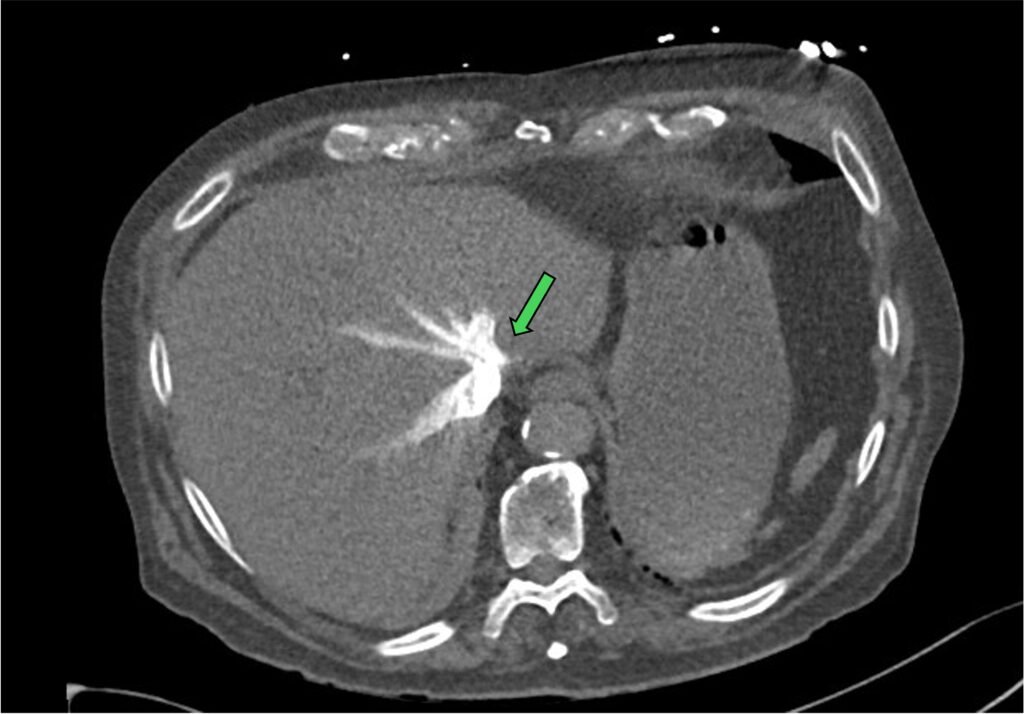
Figure 11: contrast reflux in hepatic vein
Other complications include a pulmonary infarct and pleural effusion.
While browsing the scan, it is always a good practice to look for other differentials such as pneumonia, pneumothorax etc.
The tricks & the traps !
- You can utilise multiple view / plane to distinguish an actual clots from flow artifact or vascular bifurcations.
- Proper windowing and leveling can better visualise the clot in the vessels and reduce the noise from beam hardening artifact.
- Remember, we are are not looking for a subtlety here. Its’s ok to miss the sub-sub-sub-subsegmental PE in the peripheries. But you don’t want to miss the saddle PE with RV strain and pulmonary infarct !!!
References:
- Moore AJE, Wachsmann J, Chamarthy MR, Panjikaran L, Tanabe Y, Rajiah P. Imaging of acute pulmonary embolism: an update. Cardiovasc Diagn Ther. 2018;8(3):225-243. Available from: PubMed Central https://pmc.ncbi.nlm.nih.gov/articles/PMC6039809/
- Triggiani S, Liguori C, Rinaldi R, Rella R, Rella L, Ragozzino A, et al. Comprehensive review of pulmonary embolism imaging. Insights Imaging. 2025;16(1):56. Available from: PubMed Central https://pmc.ncbi.nlm.nih.gov/articles/PMC12479586/
- Bukhari SMA, Almas T, Mufti S, Lopez R, Singh R, Tabachnik S, et al. Clinical and imaging aspects of pulmonary embolism. Curr Probl Diagn Radiol. 2025;54(3):104034. Available from: https://www.sciencedirect.com/science/article/abs/pii/S0899707124002584 (open-access via journal or institutional routes)
- American College of Radiology. ACR Appropriateness Criteria® Suspected Pulmonary Embolism. 2016 updated periodically. Available from: https://acsearch.acr.org/docs/69404/narrative/
- Jones J, Gaillard F. Pulmonary embolism. org. 2025 Jul 2 [cited 2025 Dec 31]. Available from Radiopaedia.
- Vandermeer F. CT pulmonary angiogram: pulmonary embolism, case-based approach [Internet]. YouTube; 2023 May 31 [cited 2025 Dec 31]. Available from YouTube.
- Agency for Clinical Innovation. Pulmonary thromboembolism (PE) – evaluation pathway [Internet]. NSW Government; 2023 [cited 2025 Dec 31]. Available from ACI NSW.
- Kandathil A, Chamarthy M. Pulmonary vascular anatomy & anatomical variants. Cardiovasc Diagn Ther. 2018 Jun;8(3):201-207. doi: 10.21037/cdt.2018.01.04. PMID: 30057869; PMCID: PMC6039811. Available from PubMed Central https://pmc.ncbi.nlm.nih.gov/articles/PMC6039811/
- Moore AJE, Wachsman J, Chamarthy MR, Panjikaran L, Tanabe Y, Rajjah P. Imaging og acute pulmonary embolism: an update. Cardiovasc Diagn Ther. 2018;8(3): June 27. Available from: https://cdt.amegroups.org/article/view/17831/html
Recent Posts
- Right Ventricular Dimension February 27, 2026
- Pneumothorax – CXR February 10, 2026
- The Three Planes / Views January 16, 2026
- The Hounsfield Unit, Window Level & Width January 16, 2026
- THE BLIND MEN & THE ELEPHANT January 14, 2026