
Limitation of Portable CXR
Portable Chest X-ray (CXR) in ICU vs. formal CXR in radiology suite
What are the differences? Why it matters?
Firstly, portable CXR in ICU is done in Anterior-Posterior (AP) position as compared to Posterior-Anterior. If you ask any medical student what’s the difference, the first thing they would say is the heart will appear larger in AP. Agreed.
But why / how does this happened?
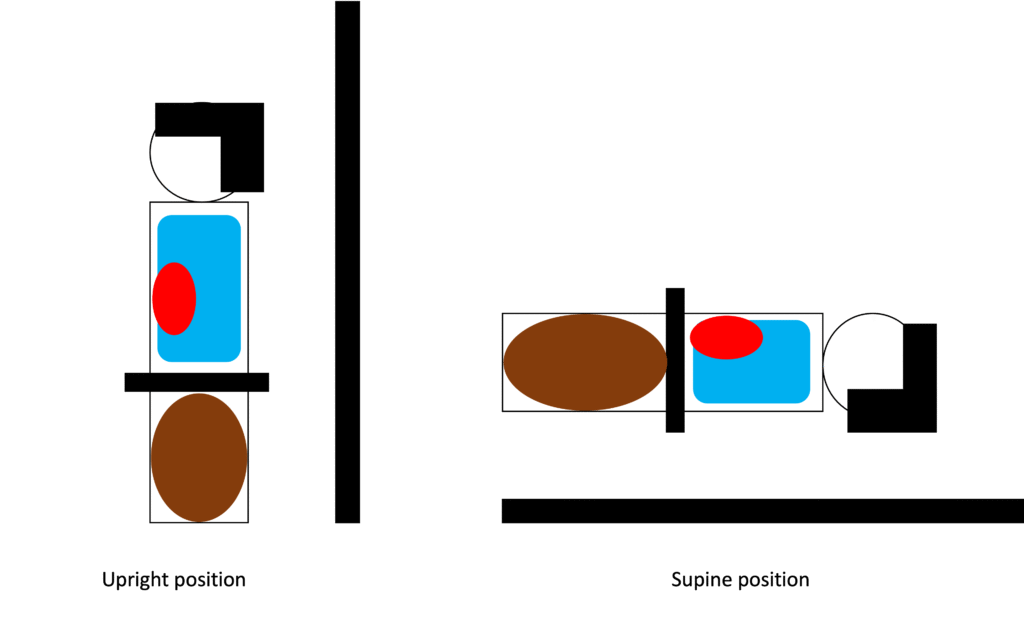
If you’re visually inclined person like me, you’ll find the image below best to explain the phenomenon.
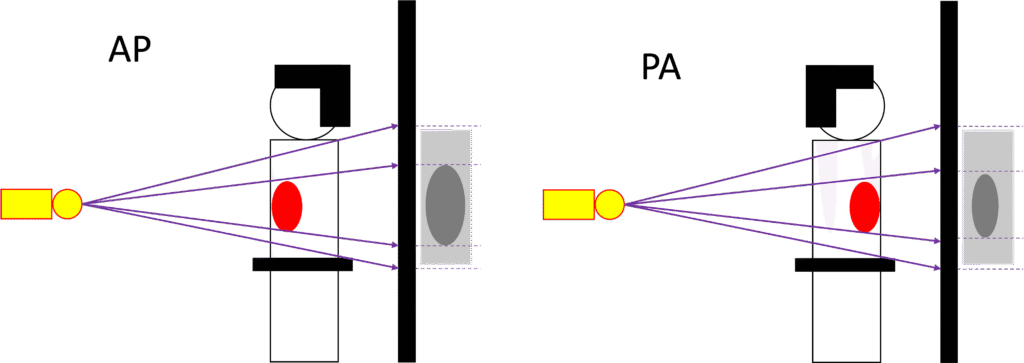
The heart is inevitably positioned closer to the x-ray source in AP position compared to PA thus creating a larger shadow on the film.
But wait, there’s more!!!
There is also difference in distance of the x-ray source and actual subject.
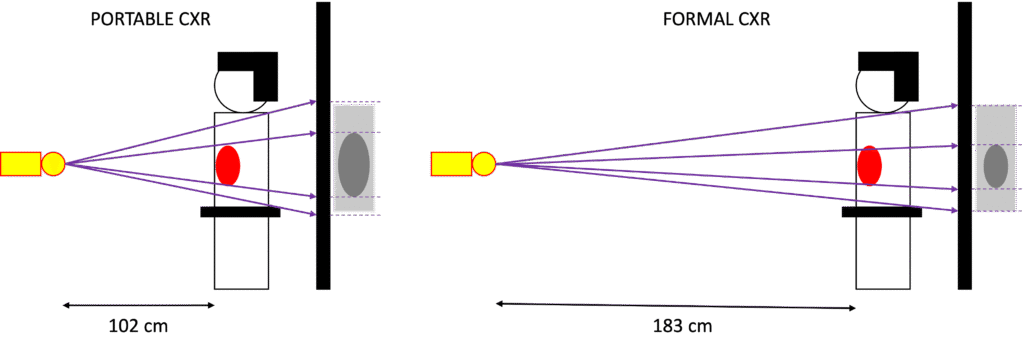
The actual technical term for this is Source-to-Image Receptor Distance (SID). According to American College of Radiology (ACR) the portable CXR should be performed at minimum SID of 40 inches (102 cm) while the formal should be performed at between SID of 40 to 72 inches (102 to 183 cm).
From the image above we can conclude that as the SID is shortened in portable CXR, the heart shadow got enlarged as well.
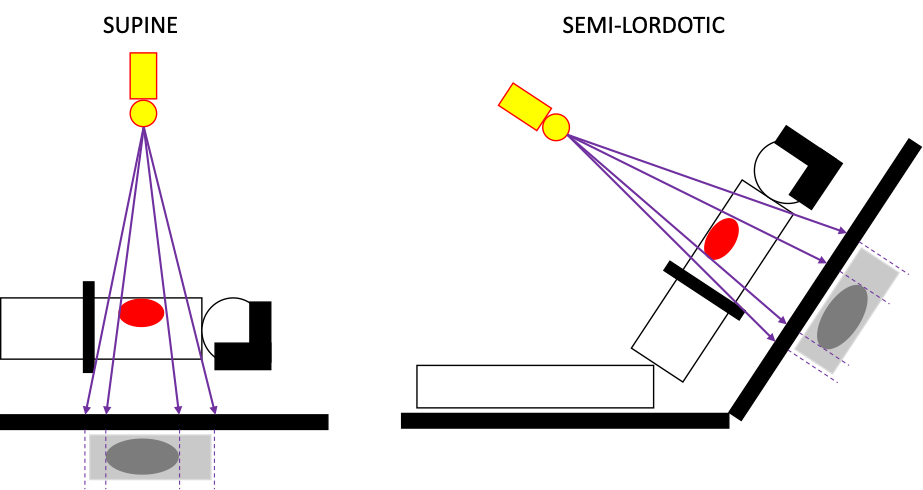
Next point, supine position.
Another major difference between portable and formal CXR is the position of the patient. For portable CXR done in ICU, the patient is almost always in supine or semi-lordotic position in bed.
Standard CXR normally done in full inspiratory phase. And there is a good reason for this. Radiologists often described this as looking for birds high on the tree.
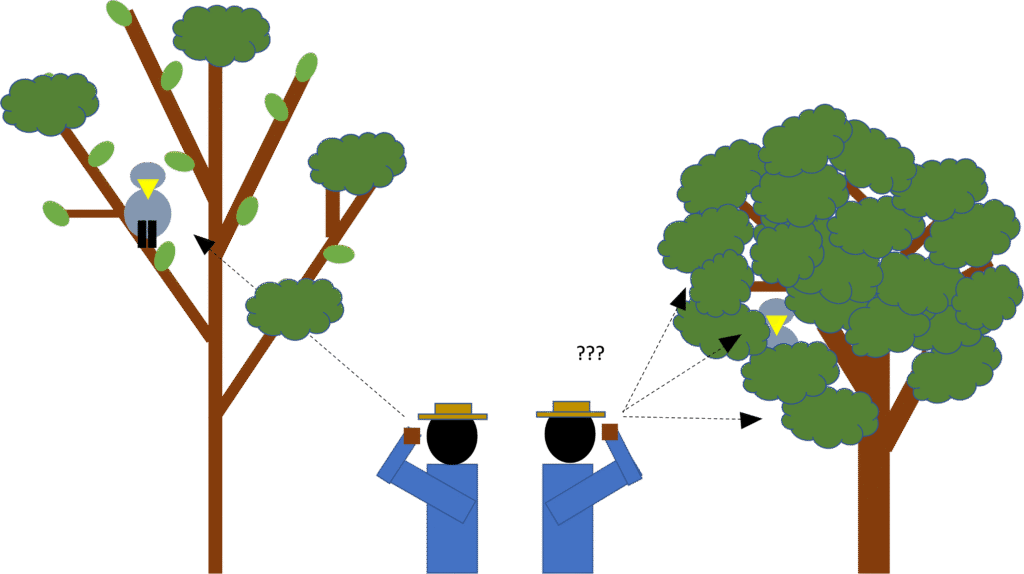
It is much easier to locate the bird if it is a widespread long branching tree rather than a crowded bush. Same principle applies here. It is much easier to identify abnormal pathology in lungs while it fully inflated.
In supine CXR, the abdominal content will push diaphragm cephalad-ly and make it harder to capture full inflated lungs.
To the next point.
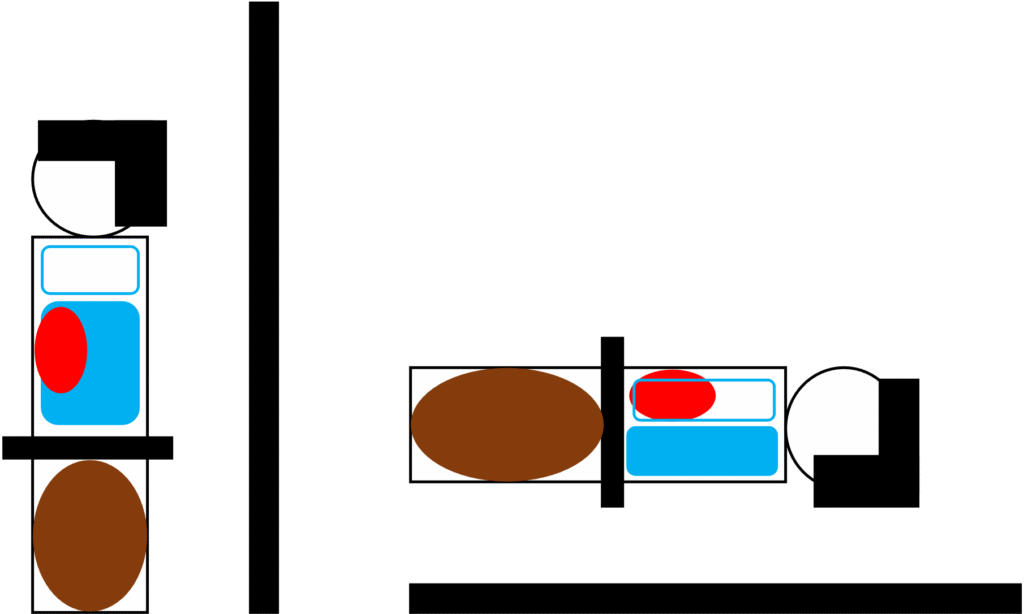
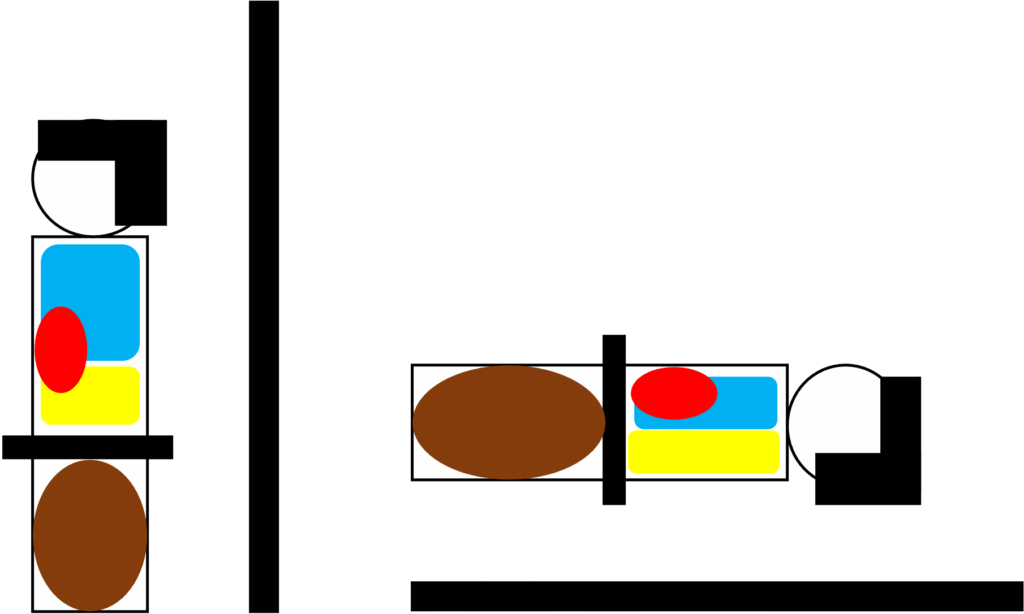
“Air goes up, fluid goes down”
In patient with pneumothorax, in supine position, the air ended up accumulated around the anterior border of the chest (rather than apical region in upright positioned patient). So you won’t be able to see the typical appearance of pneumothorax on the CXR.
Fluid in comparison behave the opposite way of the air and move downward, giving a nice air-fluid level appearance in patient in upright position. In supine patient, the fluid distributed evenly within the posterior side of the patient, giving the appearance of overall increased in opacification in the lungs.
Lastly there is an issue of angle of the xray beam.
The angle of the xray beam should ideally be 90 degree perpendicular to the patient. This is of course much easier to achieved in patient standing / sitting on a flat surface in radiology suite with the xray machine directed straight to the patient. In semi-lordotic ICU patient in bed, a good radiographer can estimate the angle of projection and act accordingly, although it is more prone to make a mistake in this scenario.
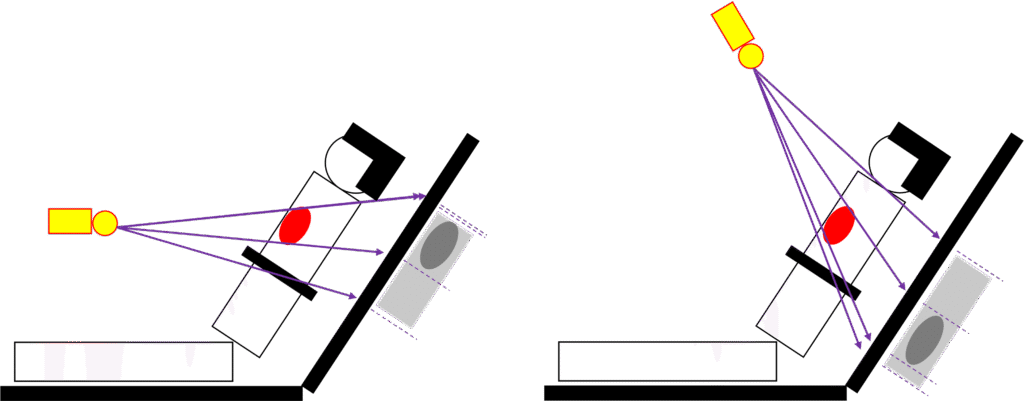
An off degree beam projection can give a distorted picture and/or even conceal the crucial pathologies underneath.
Key Points:
- AP view will make the heart and mediastium appear larger
- Supine position make it harder to get CXR with fully inflated lungs
- Pathologies like pneumothorax and effusion will not be readily visible on supine CXR
References
- Irwin RS, Lilly CM, editors. Irwin & Rippe’s Intensive Care Medicine. 7th ed. Philadelphia: Wolters Kluwer; 2012.
- Vincent JL, Abraham E, Moore FA, Kochanek PM, Fink MP, editors. Textbook of Critical Care. 7th ed. Philadelphia: Elsevier; 2017.
- Broder JS. Diagnostic Imaging for Emergency Physician. 1st North Carolina: Elsevier 2011
- Chest radiograph – PA versus AP view Radiopaedia.org; Available from: https://radiopaedia.org/articles/chest-radiograph?lang=gb
- Portable chest radiography Radiopaedia.org; Available from: https://radiopaedia.org/articles/portable-radiography?lang=gb
- American College of Radiology. ACR–SPR Practice Parameter for the Performance of Portable (Mobile Unit) Chest Radiography: American College of Radiology; updated 2023; Available from: https://gravitas.acr.org/PPTS/GetDocumentView?docId=149
- Bansal T, Beese R. Interpreting a chest X-ray. Br J Hosp Med (Lond). 2019 May 2;80(5):C75-C79. doi: 10.12968/hmed.2019.80.5.C75. PMID: 31059330. Available from: PubMed Central.
- Henschke CI, Yankelevitz DF, Wand A, Davis SD, Shiau M. Chest radiography in the ICU. Clin Imaging. 1997 Mar-Apr;21(2):90-103. doi: 10.1016/0899-7071(95)00097-6. PMID: 9095383. Available from: PubMed Central.
- Alarifi J. Benefits and Limitations of Portable Chest Radiography. Radiologic Technology. 2021 Jan;92(3):301-314. Available from: Radiologic Technology.
- Lutfallah B, Seidenwerg P. Reducing errors in portable chest radiography. Applied Radiology. 2015 Apr 7;44(4). Available from: Applied Radiology.
- Cardinale L, Volpicelli G, Lamorte A, Martino J; Andrea Veltri. Revisiting signs, strengths and weaknesses of Standard Chest Radiography in patients of Acute Dyspnea in the Emergency Department. J Thorac Dis. 2012 Aug;4(4):398-407. doi: 10.3978/j.issn.2072-1439.2012.05.05. PMID: 22934143; PMCID: PMC3426742. Available from: PubMed Central.
Recent Posts
- Right Ventricular Dimension February 27, 2026
- Pneumothorax – CXR February 10, 2026
- The Three Planes / Views January 16, 2026
- The Hounsfield Unit, Window Level & Width January 16, 2026
- THE BLIND MEN & THE ELEPHANT January 14, 2026
One thought on “Limitation of portable CXR”