
Lobar Collapse
What’s normal ?
For further details on the normal CXR please see specific section here.
For quick revision, in the normal CXR where both lungs are fully expanded, (because of the difference in tissue density) you should be able to see all sides border of the lungs, including the normal cardiomediastinal contour.
The table below described the relationship of each portion of the cardiomediastinal contour / silhouette with their respective part of the lungs.
SILHOUETTE | LUNG |
SVC / Asc Aorta | Anterior segment of RUL |
RA | Medial segment of RML |
Aortic Arch | Apical-posterior segment of LUL |
LV | Inferior segment of Lingula |
Rt Hemidiaphragm | RLL |
Lt Hemidiaphragm | LLL |
What’s not normal ?
First, there are what we called “general signs”. It tells you the consequences of the lung collapse – the volume loss. These signs include:
- Local increased in opacity (more opaque medially than laterally)
- Displacement of hilum / minor fissure (remember, you can’t see major fissure on frontal CXR)
- Elevation of diaphragm
- Mediastinal shift (towards the collapsed side)
- Compensatory hyperinflation
If you are keen to know the details, Radiopaedia done a good job explaining the specific findings of each lobe collapse. For people who tights for time, below are the simplified version of it.
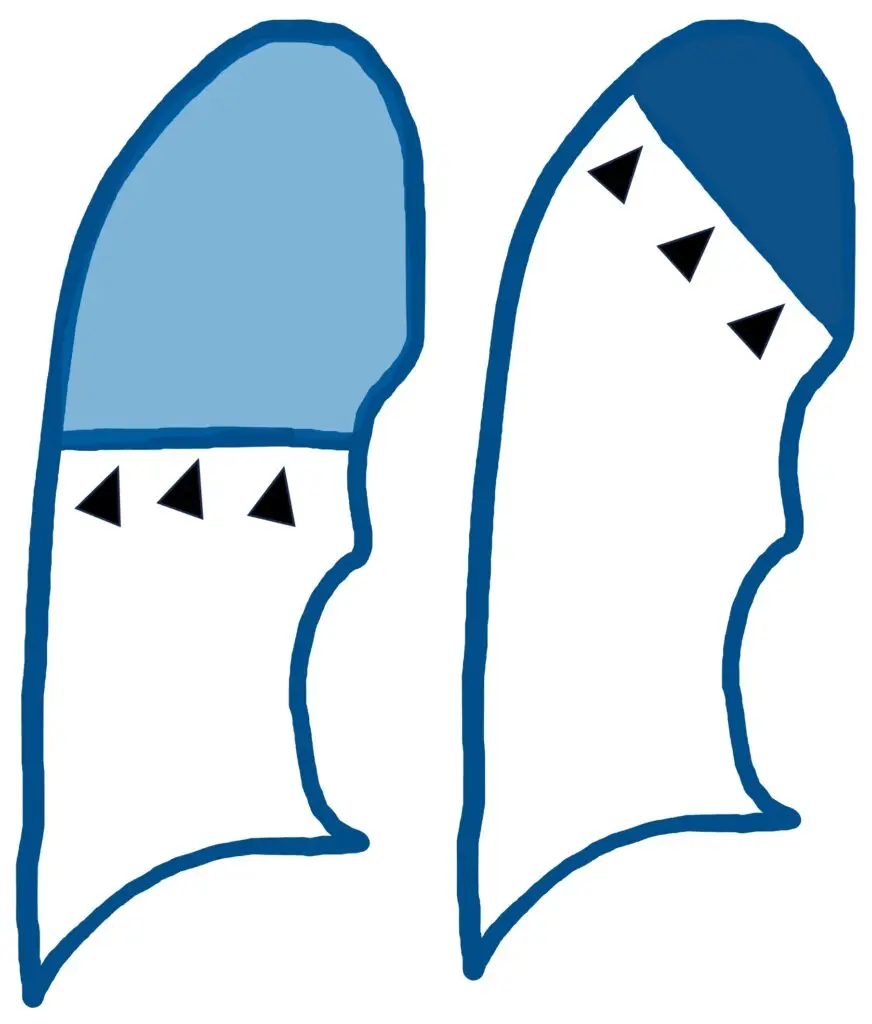
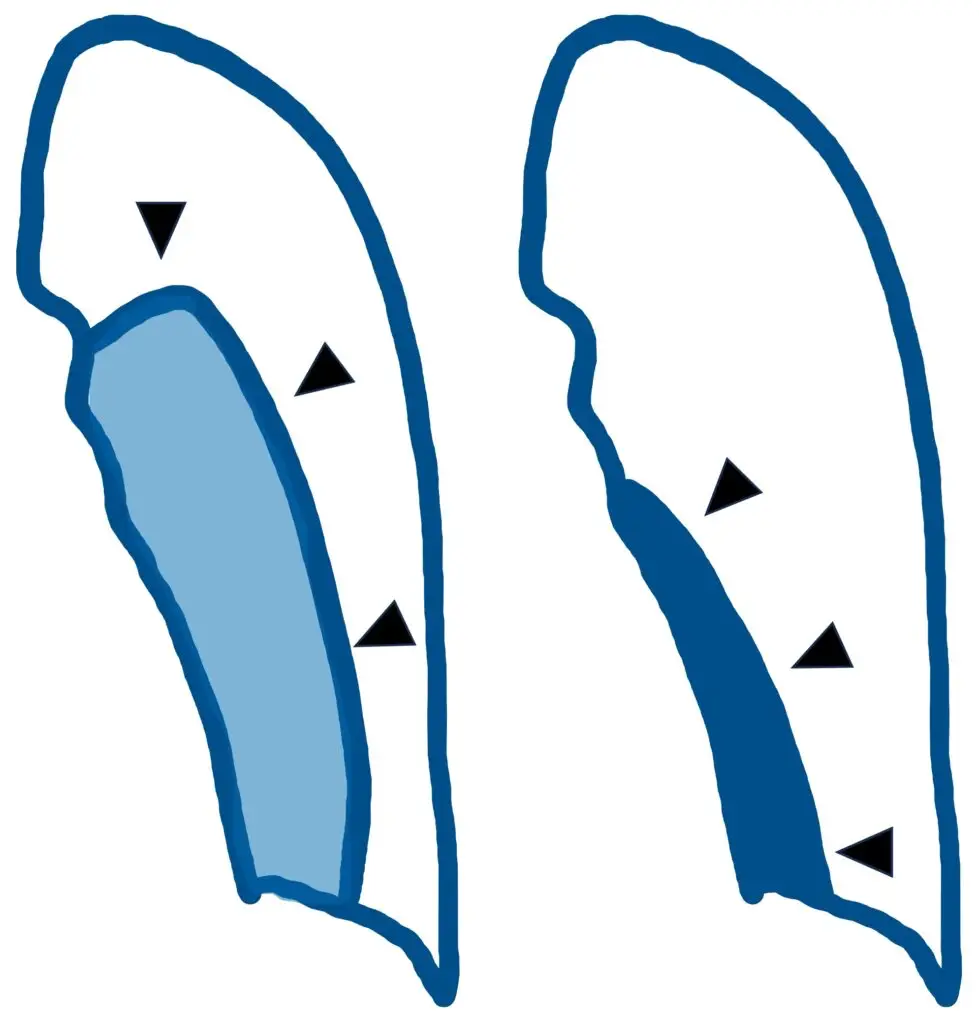
Right Upper Lobe (RUL):
- The minor fissure (and the upper lobe) collapses medially and superiorly (see black arrow)
- The SVC silhouette / right upper mediastinal border becomes more haziness and ill-defined
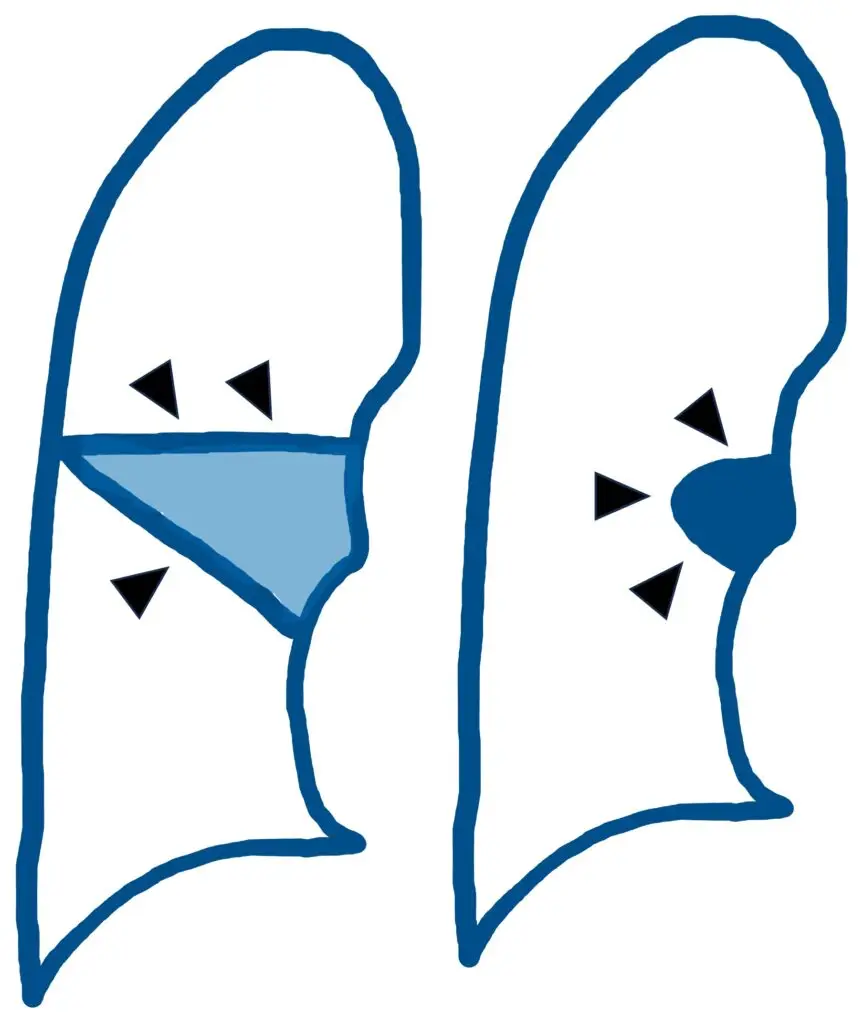
Right Middle Lobe (RML):
- The minor fissure (and the middle lobe) collapses medially and inferiorly (see black arrow)
- The right atrium border becomes more haziness and ill-defined
Right Lower Lobe (RLL):
- The lower lobe collapses medially (see black arrow) and posteriorly (you won’t be able to appreciate this on frontal XR), forming the triangle obscuring the right cardiophrenic angle
- The minor fissure merely pulled inferiorly but does not disappear and collapsed (remember, the minor fissure separates the RUL and RML, it got nothing to do with RLL)
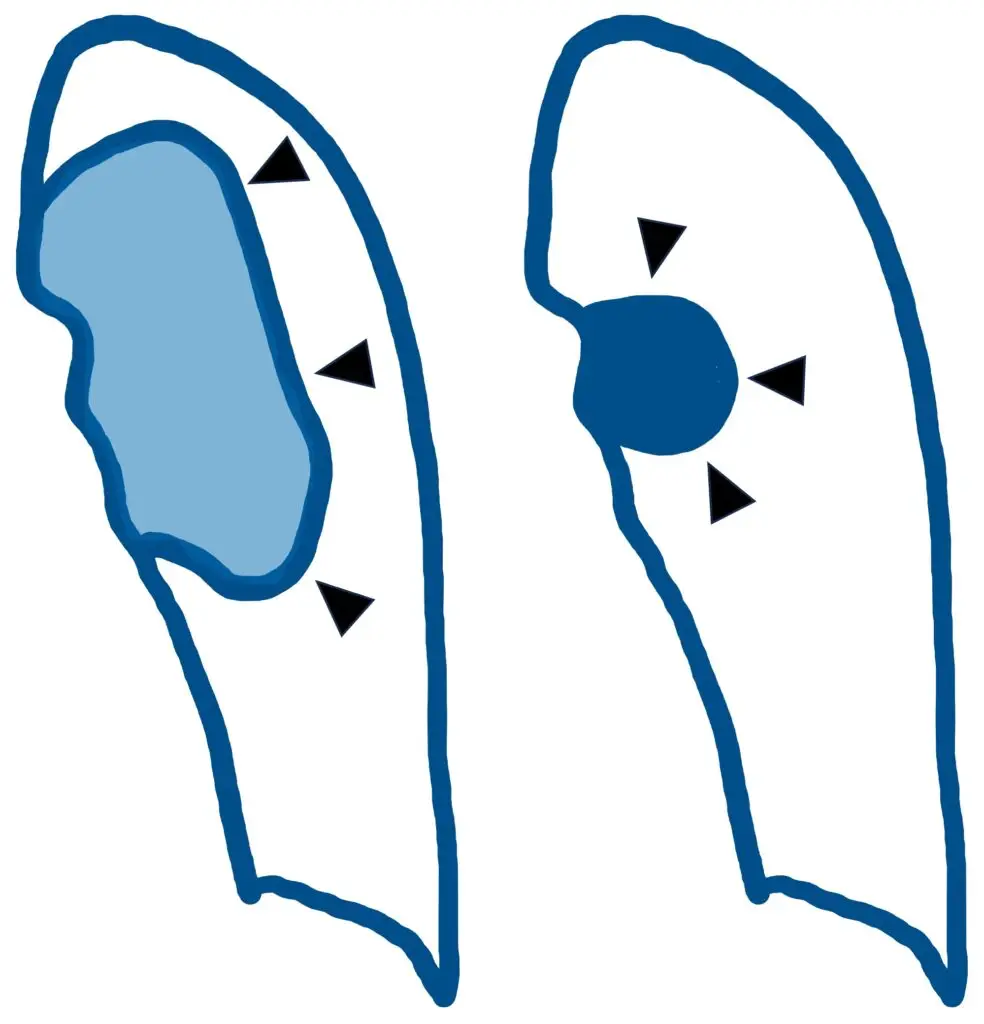
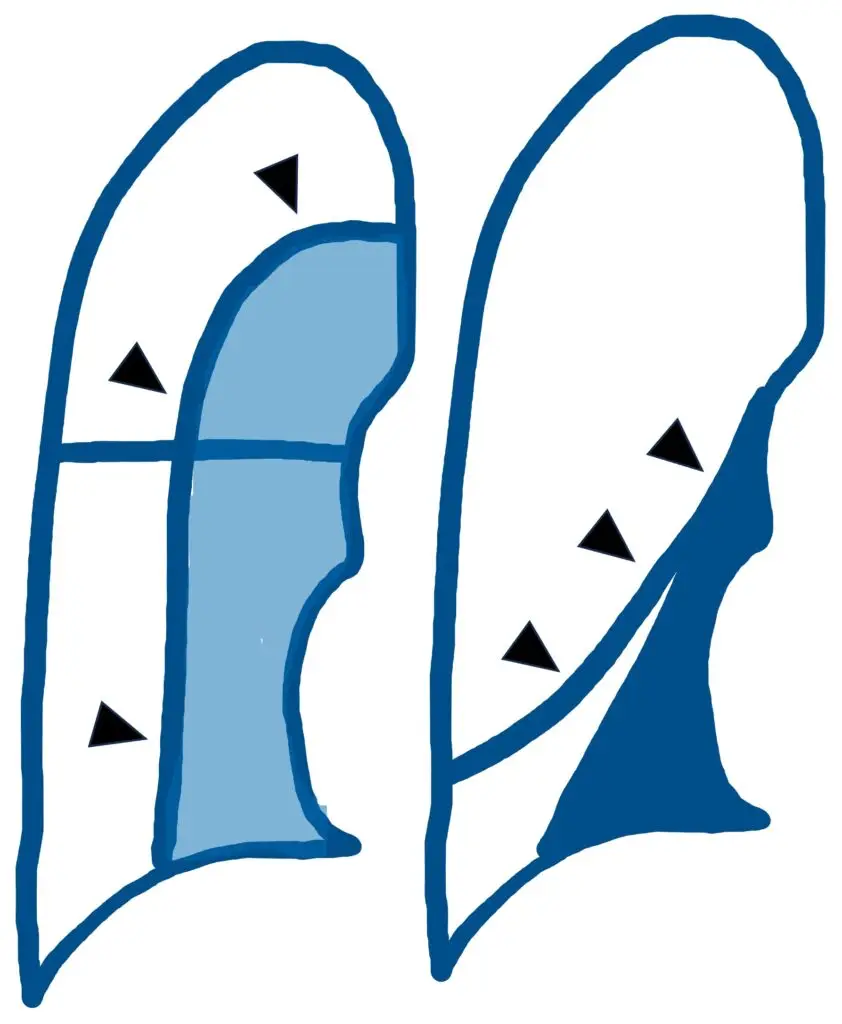
Left Upper Lobe (LUL) (often said the hardest to see on frontal CXR):
- The upper lobe collapses medially (see black arrow) and anteriorly (you won’t be able to appreciate this on frontal XR)
- The aortic arch border then becomes more haziness and ill-defined
Left Lower Lobe (LLL):
- The lower lobe collapses medially (see black arrow) and posteriorly (again, you won’t be able to appreciate this on frontal XR) forming the triangle obscuring the left cardiophrenic angle
Some interesting images for more context.
Image 1: CXR of 37 y/o intubated man with polypharmacy overdose showed RUL and RLL collapse. Hover over (or click, if you’re on portable device) to see lung re-expanded after some time on positive pressure ventilation.
Image 2: CXR of 23 y/o intubated with status epilepticus showed RML collapse. Hover over (or click, if you’re on portable device) to see lung re-expanded after some time on positive pressure ventilation.
How many features of “volume loss” can you spot from the images above ???
The tricks & the traps !
- The presence of a collapsed lung in a ICU patient often coincides with other additional conditions like pleural effusion and consolidation, don’t forget to look for these pathologies as well
- Small, partial lung collapses are often missed and to be fair, they rarely matter clinically, but it is critical not to miss a fully collapsed lung in symptomatic patient
References:
- Broder JS. Diagnostic Imaging for Emergency Physician. 1st North Carolina: Elsevier 2011
- Mancò G, Caruso V, Lezzi G, et al. Lobar collapse: what radiologists need to know. J Med Imaging Interv Radiol. 2024;11(23):1-8. Available from: https://link.springer.com/article/10.1007/s44326-024-00024-z
- Marano R, Liguori C, Savino G, Merlino B, Natale L, Bonomo L. Cardiac silhouette findings and mediastinal lines and stripes: Radiograph and CT scan correlation. Chest. 2-11;139(5):1186-1196. doi:10.1378/chest.10-0660. Available from: https://www.sciencedirect.com/science/article/pii/S0012369211602444
- Bell DJ, Jones J, et al. Lobar lung collapse. Radiopaedia.org. 2025 Dec 28. Available from: https://radiopaedia.org/articles/lobar-lung-collapse
- El-Sayed Hammad MS. Lobar collapse: basic concepts. ScienceDirect Topics. 2024. Available from: https://www.sciencedirect.com/science/article/abs/pii/0720048X96010315
- Smith C. Atelectasis – Undergraduate Diagnostic Imaging Fundamentals. Victoria (BC): Pressbooks; 2025. Available from: https://pressbooks.pub/undergradimaging/chapter/atelectasis/
- van Heesewijk J, van Kuijk C, van Langevelde K. Chest X-Ray – Lung disease. The Radiology Assistant. 2024. Available from: https://radiologyassistant.nl/chest/chest-x-ray/lung-disease
- Radiology Key. Pulmonary lobar collapse. Radiology Key: Fastest Radiology Insight Engine. 2024. Available from: https://radiologykey.com/pulmonary-lobar-collapse-2/
- Radiology Masterclass. Chest X-ray abnormalities: lung abnormalities. 2026. Available from: https://www.radiologymasterclass.co.uk/tutorials/chest/chest_pathology/chest_pathology_page3
- Kanne JP. A systematic approach to chest radiographic analysis. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2025. Available from: https://www.ncbi.nlm.nih.gov/books/NBK553874/
Recent Posts
- Piezo 101: Squeezing Electricity Since 1880 April 16, 2026
- Central Venous Access Device (CVAD) April 11, 2026
- Pneumonia – CXR March 28, 2026
- Right Ventricular Systolic Function March 7, 2026
- Right Ventricular Dimension February 27, 2026