
Pneumothorax - CXR
What’s normal ?
There is not much else to say here. You would expect in a normal CXR with full lungs expansion, you will see the vasculature and bronchial marking spread evenly to the edge of the chest wall bilaterally.
What’s not normal ?
In CXR with pneumothorax you will see a visceral pleural edge with no lung markings peripheral / lateral to this line. As the ‘bubble’ getting bigger, you may see other accompanied features (see Figure 2) including:
- Mediastinal shift away from the affected side (red arrows)
- Ipsilateral diaphragm depression (green arrows)
- Peripheral area appears more radiolucent than adjacent lung
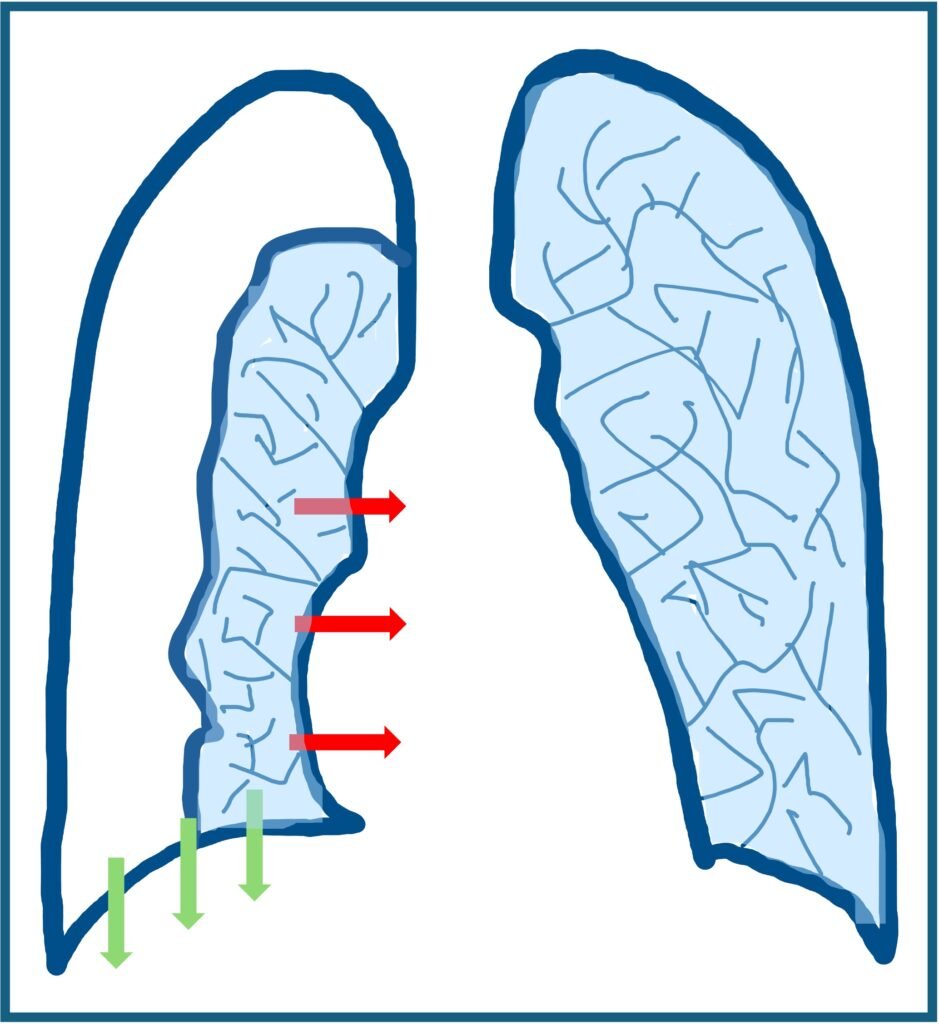
Figure 2: features of pneumothorax on chest x-ray
Now that you are convinced there is a pneumothorax, you need to find out:
- What kind of pneumothorax is it?
- How bad is it?
- Are there any other pathologies / complications there as well?
Types of pneumothorax
- (Primary) spontaneous pneumothorax (PSP)
There are certain group of people that are genetically prone to developed spontaneous pneumothorax. They do not have chronic underlying lung disease and often exhibit a tall and thin body habitus.
Image 1: CXR of 30 years old man with no known chronic lung disease, presented to ED with sudden onset central chest pain. The green line showed the visceral pleural edge, with no visible vascular / bronchial marking on the lateral / peripheral side
- (Secondary) spontaneous pneumothorax (SSP)
This category of patients has an established chronic lung disease. They will often have other signs of chronic lung disease on the CXR such as emphysematous changes, hyperinflation etc.
Why do we care? Because both PSP and SSP have their own separate flow chart management.
- Traumatic / iatrogenic pneumothorax
As the name suggested, it does not happen spontaneously. A traumatic pneumothorax may be caused by pulmonary laceration, rib fracture, oesophageal rupture, etc. Based on additional history and examination, the patient may require further imaging or urgent intervention.
An iatrogenic pneumothorax may be caused by NGT / CVC insertion, lung biopsy, CPR, etc. In this case, early recognition and correction of a malpositioned NGT, for example, is essential.
Image 2: CXR of 67 years old man post out of hospital cardiac arrest. The green line showed the visceral pleural edge. Also noted the ribs fracture (red lines) likely secondary to CPR and the subcutaneous emphysema (blue arrows). Other findings include the presence of ETT and left IJV CVC.
- Tension pneumothorax
Tension pneumothorax is a life-threatening emergency and a clinical diagnosis. You don’t need an x-ray to tell you this!
Quantifying the pneumothorax
Once you identify it, the next thing your senior going to ask is how big it is. Because you might need to drain it. There are plenty of methods to quantify this. Some may be more accurate and reliable than others. Below are some of methods on how to measure it.
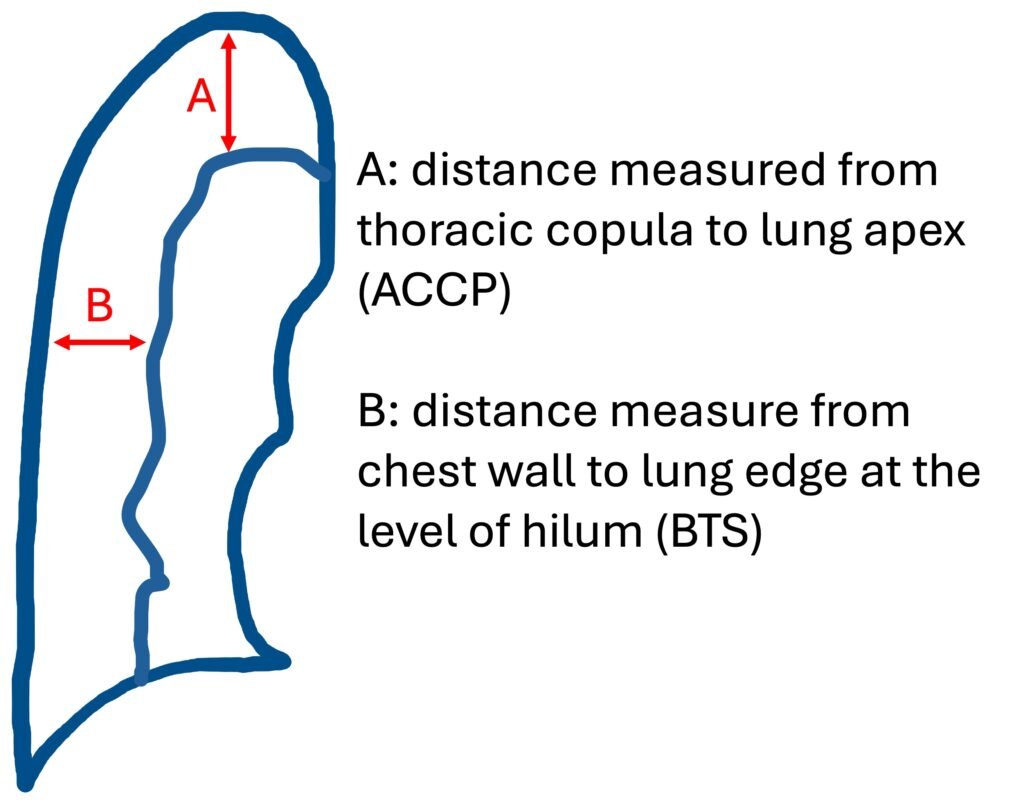
- American College of Chest Physicians (ACCP) guidelines
Distance measured from thoracic cupola to lung apex (A)
- British Thoracic Society (BTS) guidelines
Distance measured from chest wall to lung edge at the level of the hilum (B)
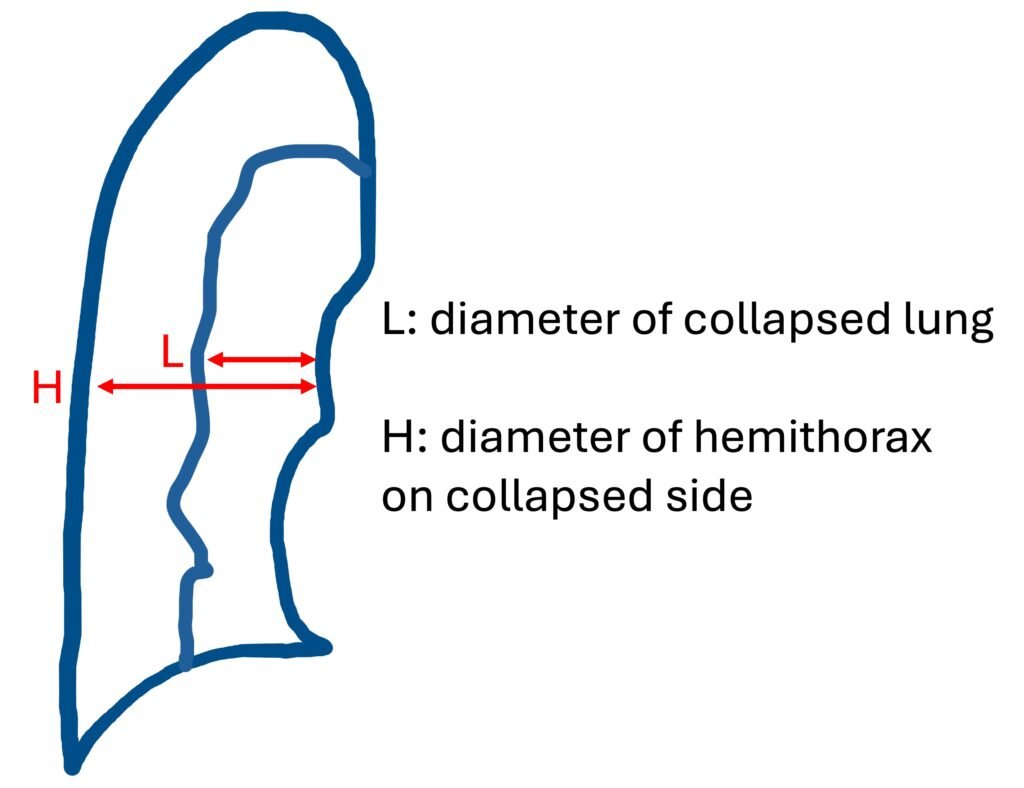
- Light Index
The estimated pneumothorax percentage = (1 − L3/H3) × 100; where H = hemithorax diameter and L = diameter of the collapsed lung
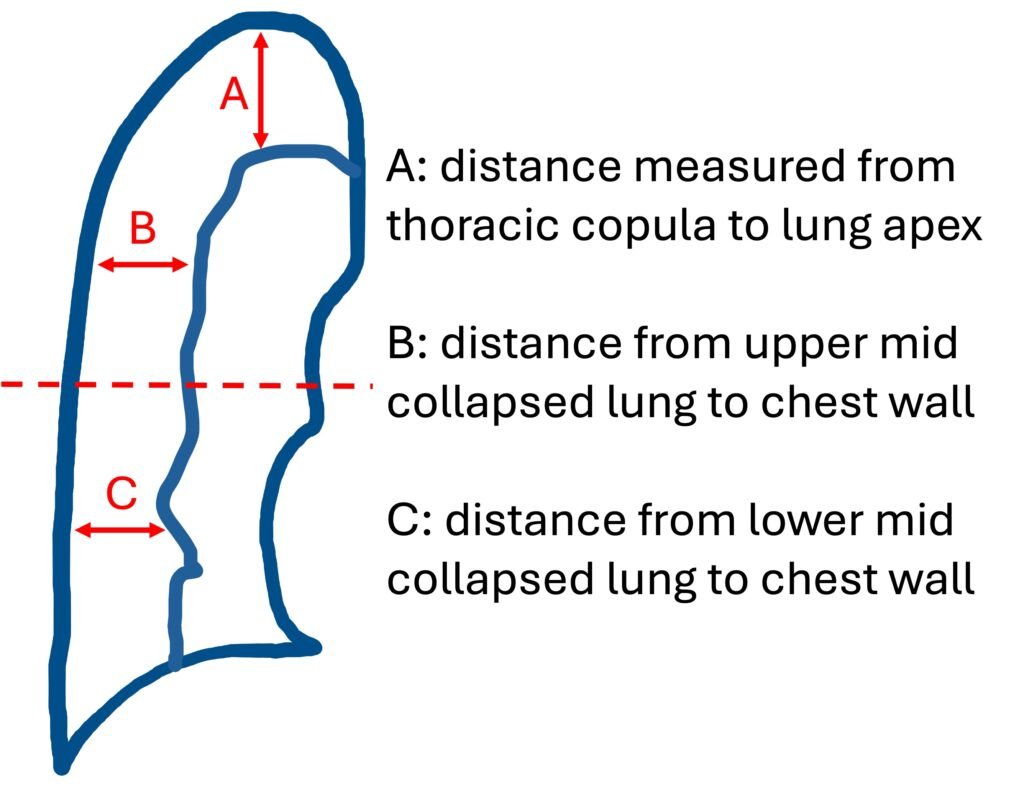
- Rhea method
Average interpleural distances (AID): [A+B+C]/3
The percentage of pneumothorax can be estimated based on the AID using the nomogram (see link)
- Collins method
Pneumothorax Volume Percentage = 4.2 + [4.7 x (A+ B + C)]
Below are the cut-off threshold for large pneumothorax for each of the methods mentioned above.
- BTS: > 2 cm
- ACCP: > 3 cm
- Light Index: > 20%
- Collin Method: > 32% or in simple term A+B+C > 6 cm
So which one is the most accurate? It is in general agreement that Collins Method is the most accurate method because it is derived from the helical CT scan volumetric data. It also offers inter- and intra-rater reliability in clinical settings.
The trips & the traps !
- Pneumothorax in supine patient
In supine patient, as discussed here, the air bubble tends to hover above the lung parenchymal thus obscuring it on the x-ray. In some cases, you might be able to see the “deep sulcus sign”. If I can find a nice picture of this “deep sulcus sign” in the future, I will surely put it here.
- Mimics of pneumothorax
Be mindful of the mimics of pneumothorax. Most common mimics include a skin fold, scapular margins and a companion shadows along inferior margin of the ribs. Just remember, in mimics, you can always see the lung vasculature on both side of the line.
Image 3: Another CXR with the green line showed the scapular margin. Note that you can still see the vasculature marking on both side of the line.
References:
- Gorrochategui M, Feger J, Silverstone L, et al. Reference article, Radiopaedia.org https://doi.org/10.53347/rID-4578
- Herring W. Recognizing pneumothorax, pneumomediastinum, pneumopericardium, and subcutaneous emphysema. Radiology Assistant [Internet]. 2021 Available from: https://radiologyassistant.nl/chest/chest-x-ray/basic-interpretation#pleura-pneumothorax
- MacDuff A, Arnold A, Harvey J. Management of spontaneous pneumothorax: British Thoracic Society pleural disease guideline 2010. Thorax [Internet]. 2010-65(Suppl 2):ii18-ii31. Available from: brit-thoracic.org.uk
- Roberts ME, Rahman NM, Agrawal A, Akulian J, Belcher E, Bertolaccini L, et al. British Thoracic Society Guideline for pleural disease. 2023;78(11):1143-1156.
- Khan AN. Demystifying the persistent pneumothorax: role of imaging. Insights Imaging. 2016;7(3):411-429.
- Aguinagalde, Borja PhD*; Zabaleta, Jon PhD*; López, Iker PhD*; Izquierdo, Jose M. PhD*; Mendoza, Mikel MD†; Garmendia, Eñaut MD†; Fernandez-Monge, Arantza MD*; Lizarbe, Jon A. MD*. Quantification of Pneumothorax Volume on Chest X-Ray: A More Accurate Index Based On Measurements Made With 3D-printed Models. Journal of Thoracic Imaging 37(4):p 262-268, July 2022. | DOI: 10.1097/RTI.0000000000000636
- Louw EH, Shaw JA, Koegelenberg CFN. New insights into spontaneous pneumothorax: A review. Afr J Thorac Crit Care Med. 2021 Mar 9;27(1):10.7196/AJTCCM.2021.v27i1.054. doi: 10.7196/AJTCCM.2021.v27i1.054. PMID: 34240041; PMCID: PMC8203058.
- Salazar AJ, Aguirre DA, Ocampo J, Camacho JC, Díaz XA. Evaluation of three pneumothorax size quantification methods on digitized chest X-ray films using medical-grade grayscale and consumer-grade color displays. J Digit Imaging. 2014 Apr;27(2):280-6. doi: 10.1007/s10278-013-9651-2. PMID: 24149967; PMCID: PMC3948932.
- StatPearls [Internet]. Acute Pneumothorax Evaluation and Treatment. Treasure Island (FL): StatPearls Publishing; 2024.
- Pneumothorax Percentage Calculator (Collins and Light Methods). RadioGyan: Radiology Resources. 2024.
- Kelly AM, Weldon D, Tsang AY, Graham CA. Comparison between two methods for estimating pneumothorax size from chest X-rays. Respir Med. 2006 Aug;100(8):1356-9. doi: 10.1016/j.rmed.2005.11.022. Epub 2006 Jan 6. PMID: 16406560.
- Collins CD, Lopez A, Mathie A, Wood V, Jackson JE, Roddie ME. Quantification of pneumothorax size on chest radiographs using interpleural distances: regression analysis based on volume measurements from helical CT. AJR Am J Roentgenol. 1995 Nov;165(5):1127-30. doi: 10.2214/ajr.165.5.7572489. PMID: 7572489.
Recent Posts
- Piezo 101: Squeezing Electricity Since 1880 April 16, 2026
- Central Venous Access Device (CVAD) April 11, 2026
- Pneumonia – CXR March 28, 2026
- Right Ventricular Systolic Function March 7, 2026
- Right Ventricular Dimension February 27, 2026